This lecture by Dr. Kent VanTyle occurred on (put weekday, date, and month of lecture(s)).
Back to RX 411 - Principles of Drug Action
Study Materials[]
Required reading:
Handouts:
Panopto:
Objectives[]
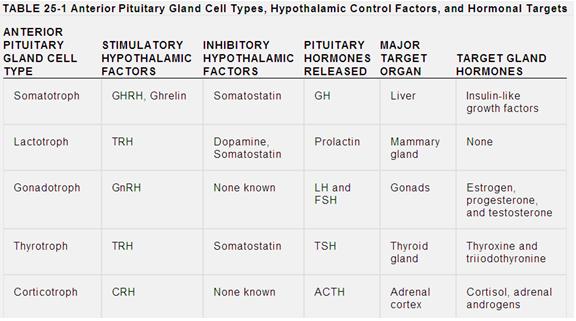
Identify the control processes, target glands, and target gland hormone products for each of the anterior pituitary hormones[]
There are 5 basic hormones produced by the anterior pituitary. The hypothalamus largely stimulates or inhibits the release of these hormones.
- Growth Hormone - is released from somatotroph cells when they are stimulated by Growth Hormone Releasing Hormone (GHRH) or Gherlin. It goes on to act on the liver, which produces Insulin-like growth factors in response to GH. Somatostatin inhibits the release of GH.
- Prolactin - is released from lactotroph cells when they are stimulated by Thyrotropic Releasing Hormone. It goes on to act on the Mammary glands. Dopamine and Somatostatin inhibit the release of prolactin.
- Leuteinizing Hormone and Follicle Stimulating Hormone - are released from gonadotroph cells when they are stimulated by Gonadotropin Releasing Hormone. It goes on to act at the gonads, which releases Estrogen, Progesterone, and Testosterone in response to LH and FSH. There are no known hypothalamic inhibitory factors for LH and FSH.
- Thyroid stimulating hormone - is released from Thyrotroph cells when they are stimualted by Thyrotropic Releasing Hormone. It goes on to act on the thyroid gland, which releasing Thyroxine and Triiodothyronine in response to TSH. Somatostatin inhibits the release of TSH.
- Adrenocorticotropic Hormone - is released from corticotroph cells when they are stimulated by Corticotropin Releasing Hormone. It goes on to act on the adrenal cortex, which makes Cortisol and adrenal androgens in response to ACTH. There are no known hypothalamic inhibitory factors for ACTH
Identify the commercial products available for each of the anterior/posterior pituitary hormones.[]
Growth hormone Deficiency Treatment[]
The standard for growth hormone deficiency treatment is somatropin. However, Laron Dwarfs have a resistance to GH treatment, so they need Mecasermin instead
Growth Hormone
- Somatropin - composed of 191 amino acids. More commonly given. Dosed once a day and injected subcutaneously in the evening (since GH is normally spiked in the evening when someone sleeps. Given until a child quits growing due to long bone epiphyseal plate closure. There's no evidence that giving it into adulthood has any value. An expensive drug.
- plasma half life is 20 minutes, biological half life of 9-17 hours
- growth hormone is abused to increase muscle mass. There are no studies to show its benefit however
- Somatrem - composed of 192 amino acids. Similar effects to Somatropin
Growth Hormone Releasing Hormone
- Sermorelin - has no advantage over GH in GH deficient children
IGF-1
- Mecasermin - indicated only for Laron Syndrome (GH resistance due to mutations in GH receptor) no studies to show superiority to GH in GH deficient patients.
Acromegaly (GH excess) Treatment[]
Somatostatin Analogues can typically help treat a tumor that is secreting GH, although if surgical removal is possible that may be another option. Reversing sxs of soft tissue overgrowth is usually not possible, but returning metabolic activity to normal and reversing insulin resistance is a viable outcome.
Octreotide (SandostatinLAR) -
- given 1x can normalize GH in 75% of patients with a GH secreting adenoma of the pituitary (acromegaly)
- may not decrease tumor size, shrinks tumor,
- unfortunately the physical symptoms of acromegaly can not be reversed completely
- there will be some reduction in soft tissue overgrowth (size of tongue, lips, etc)
Pegvisomant
- (GH receptor competitive antagonist)
- when given for 1 year, 97% had normal IGF-1
- does not shrink tumor, may increase in size
- plasma glucose needs to be monitored, as GH decreases plasma glucose should decrease, there is a possibility of severe hypoglycemia